DEFINITION
Breast cancer starts when cells in the breast begin to grow out of control. These
cells usually form a tumor that can often be seen on an x-ray or felt as a
lump. The tumor is malignant (cancer) if the cells can grow into (invade)
surrounding tissues or spread (metastasize) to distant areas of the body. Breast
cancer occurs almost entirely in women, but men can get breast cancer, too.
Cells in nearly any part of the body can become cancer and can spread to other areas of
the body. To learn more about what is cancer and how all cancers start and
spread, see our section on Cancer Basics.
cells usually form a tumor that can often be seen on an x-ray or felt as a
lump. The tumor is malignant (cancer) if the cells can grow into (invade)
surrounding tissues or spread (metastasize) to distant areas of the body. Breast
cancer occurs almost entirely in women, but men can get breast cancer, too.
Cells in nearly any part of the body can become cancer and can spread to other areas of
the body. To learn more about what is cancer and how all cancers start and
spread, see our section on Cancer Basics.
ILLUSTRATION
FREQUENCY
Number of New Cases and Deaths per 100,000: The number of new cases of female breast cancer was 125.0 per 100,000 women per year. The number of deaths was 21.5 per 100,000 women per year. These rates are age-adjusted and based on 2009-2013 cases and deaths.
Lifetime Risk of Developing Cancer: Approximately 12.4 percent of women will be diagnosed with female breast cancer at some point during their lifetime, based on 2011-2013 data.
Prevalence of This Cancer: In 2013, there were an estimated 3,053,450 women living with female breast cancer in the United States.
Lifetime Risk of Developing Cancer: Approximately 12.4 percent of women will be diagnosed with female breast cancer at some point during their lifetime, based on 2011-2013 data.
Prevalence of This Cancer: In 2013, there were an estimated 3,053,450 women living with female breast cancer in the United States.
DIAGNOSIS AND MANAGEMENT
Doctors use many tests to diagnose cancer and find out if the cancer has spread or metastasized to other parts of the body beyond the breast and the lymph nodes under the arm. Some tests may also help the doctor decide which treatments may be the most effective. For most types of cancer, a biopsy is the only way to make a definitive diagnosis of cancer. A biopsy is the removal of a small amount of tissue or cells for examination under a microscope. See below for more information about the types of biopsies that can be performed. If a biopsy is not possible, the doctor may suggest other tests that will help make a diagnosis. Imaging tests may be used to find out whether the cancer has spread.
This list describes options for diagnosing this type of cancer, and not all tests listed will be used for every person. Your doctor may consider these factors when choosing a diagnostic test:
The following tests may be used to diagnose breast cancer or for follow-up testing after the cancer has been diagnosed. Not every person will need all of these tests.
Imaging testsThe following imaging tests may be done to learn more about a suspicious area found in the breast during screening.
Genomic tests to predict recurrence riskTests that take an even closer look at the biology of the tumor are commonly used to understand more about a woman’s breast cancer, particularly for a cancer that has not spread to other organs. These tests can help estimate the risk of cancer recurrence in the years after diagnosis. They can also predict whether a treatment will be helpful to reduce the risk of cancer recurrence. This helps some patients avoid the possible side effects of a treatment that is not likely to work well.
The tests described below are typically done on tissue removed during surgery. Most patients will not need an extra biopsy or more surgery. For more information about genomic tests, what they mean, and how the results might affect your treatment plan, talk with your doctor.
Breast cancer treatment takes different approaches depending on the conditions. The mainstay of breast cancer treatment is surgery when the tumor is localized, followed by chemotherapy (when indicated), radiotherapy, and, for ER-positive tumours, adjuvant hormonal therapy (with tamoxifen or an aromatase inhibitor). Management of breast cancer is undertaken by a multidisciplinary team based on national and international guidelines. Depending on clinical criteria (age, type of cancer, size, presence or absence of metastasis) patients are roughly divided to high risk and low risk cases, with each risk category following different rules for therapy. Treatment possibilities include radiation therapy, chemotherapy, hormone therapy, and immune therapy
This list describes options for diagnosing this type of cancer, and not all tests listed will be used for every person. Your doctor may consider these factors when choosing a diagnostic test:
- Age and medical condition
- Type of cancer suspected
- Signs and symptoms
- Previous test results
The following tests may be used to diagnose breast cancer or for follow-up testing after the cancer has been diagnosed. Not every person will need all of these tests.
Imaging testsThe following imaging tests may be done to learn more about a suspicious area found in the breast during screening.
- Diagnostic mammography. Diagnostic mammography is similar to screening mammography except that more pictures of the breast are taken, and it is often used when a woman is experiencing signs, such as a new lump or nipple discharge. Diagnostic mammography may also be used if something suspicious is found on a screening mammogram.
- Ultrasound. An ultrasound uses high-frequency sound waves to create an image of the breast tissue. An ultrasound can distinguish between a solid mass, which may be cancer, and a fluid-filled cyst, which is usually not cancer.
- MRI. An MRI uses magnetic fields, not x-rays, to produce detailed images of the body. An MRI can also be used to measure the tumor’s size. A special dye called a contrast medium is given into the patient’s vein before the scan to help create a clear picture of the possible cancer. A breast MRI may be used after a woman has been diagnosed with cancer to check the other breast for cancer or to find out how much the disease has grown throughout the breast. It may also be used for screening, along with mammography, for some women with a very high risk of developing breast cancer (see Prevention).
- A fine needle aspiration biopsy uses a thin needle to remove a small sample of cells.
- A core needle biopsy uses a wider needle to remove a larger sample of tissue. This is usually the preferred biopsy technique for finding out whether an abnormality on a physical examination or an imaging test is cancer. A vacuum-assisted biopsy removes several large cores of tissue. Local anesthesia, which is medication to block pain, is used to lessen a patient’s discomfort during the procedure.
- A surgical biopsy removes the largest amount of tissue. This biopsy may be incisional, which is the removal of part of the lump, or excisional, which is the removal of the entire lump. Because surgery is best done after a cancer diagnosis has been made, a surgical biopsy is usually not the recommended way to diagnose breast cancer. Most often, non-surgical core needle biopsies are recommended to diagnose breast cancer. This means that only one surgical procedure is needed to remove the tumor and to take samples of the lymph nodes.
- Image-guided biopsy is used when a distinct lump cannot be felt, but an abnormality is seen with an imaging test, such as a mammogram. During this procedure, a needle is guided to the location with the help of an imaging technique, such as mammography, ultrasound, or MRI. A stereotactic biopsy is done using mammography to help guide the needle. A small metal clip may be put into the breast to mark where the biopsy sample was taken, in case the tissue is cancerous and more surgery is needed. This clip is usually titanium so it will not cause problems with future imaging tests, but check with your doctor before you have additional imaging tests. An image-guided biopsy can be done using a fine needle, core, or vacuum-assisted biopsy (see above), depending on the amount of tissue being removed. Imaging tests may also be used to help do a biopsy on a lump that can be felt, in order to help find the best location.
- Sentinel lymph node biopsy is a way to find out if there is cancer in the lymph nodes near the breast. Learn more about sentinel lymph node biopsy in the Treatment Options section.
- Tumor features. Examination of the tumor under the microscope is used to determine if it is invasive or in situ, ductal or lobular, and whether the cancer has spread to the lymph nodes. The margins or edges of the tumor are also examined and their distance from the tumor is measured, which is called margin width.
- ER and PR. Testing for ER and PR (see Overview) helps determine both the patient’s risk of recurrence and the type of treatment that is most likely to lower the risk of recurrence. ER and PR are often measured for DCIS as well. Generally, hormonal therapy (see Treatment Options) works well for ER-positive and/or PR-positive cancers. Learn about ER and PR testing recommendations from ASCO and the College of American Pathologists (CAP).
- HER2. The HER2 status (see Overview) helps determine whether drugs that target the HER2 receptor, for example the antibody treatment trastuzumab (Herceptin), might help treat the cancer. In addition, about 50% of HER2-positive tumors also have hormone receptors and can benefit from both hormone and HER2 directed therapy. Read ASCO’s and CAP's recommendations for HER2 testing for breast cancer
- Grade. The tumor grade is also determined from a biopsy. Grade refers to how different the cancer cells look from healthy cells, and whether they appear slower growing or faster growing. There are three grades: grade 1 (well differentiated), grade 2 (moderately differentiated), and grade 3 (poorly differentiated).
Genomic tests to predict recurrence riskTests that take an even closer look at the biology of the tumor are commonly used to understand more about a woman’s breast cancer, particularly for a cancer that has not spread to other organs. These tests can help estimate the risk of cancer recurrence in the years after diagnosis. They can also predict whether a treatment will be helpful to reduce the risk of cancer recurrence. This helps some patients avoid the possible side effects of a treatment that is not likely to work well.
The tests described below are typically done on tissue removed during surgery. Most patients will not need an extra biopsy or more surgery. For more information about genomic tests, what they mean, and how the results might affect your treatment plan, talk with your doctor.
- Oncotype Dx™. This test evaluates 16 cancer-related genes and 5 reference genes to estimate the risk of the cancer coming back in a place other than the breast and nearby lymph nodes within 10 years after diagnosis for women with stage I or stage II (see Stages) ER-positive breast cancer treated with hormonal therapy alone. Results are mainly used to help make decisions about whether chemotherapy should be added to a person’s treatment with hormonal therapy. Although this test is typically used for patients with breast cancer that has not spread to the lymph nodes, recent research suggests that this test may be useful for some patients with cancer that has spread to the lymph nodes.
- Mammaprint™. This test uses information from 70 genes to predict the risk of the cancer coming back for early-stage, low-risk breast cancer. It is approved by the FDA for estimating the risk of recurrence in early-stage breast cancer, but it is not yet known if this test can predict whether chemotherapy will work. This test is more common in Europe than in the United States.
- Additional tests. Other tests are being researched and may become additional tools to guide treatment options in the future. These tests include the following, among others:
- Breast cancer index (BCI)
- Prosigna™ (PAM50)
- Complete blood count. A complete blood count (CBC) is used to measure the number of different types of cells, such as red blood cells and white blood cells, in a sample of a person’s blood. It is done to make sure that your bone marrow is functioning well.
- Serum chemistry. These tests are often done to look at minerals in your blood, such as potassium and calcium, called electrolytes and specialized proteins called enzymes that can be abnormal if cancer has spread. However, many noncancerous conditions can cause changes in these tests, and they are not specific to cancer.
- Alkaline phosphatase is an enzyme that can be associated with disease that has spread to the liver, bone, or bile ducts.
- Blood calcium levels can be high if cancer has spread to the bone.
- Total bilirubin count and the enzymes alanine aminotransferase (ALT) and aspartate aminotransferase (AST) evaluate liver function. High levels of any of these substances can indicate liver damage, a sign that the cancer may have spread to that organ.
- Hepatitis tests. These may be used to check for evidence of prior exposure to hepatitis B and/or hepatitis C. If you have evidence of an active hepatitis B infection, you may need to take a special medication to suppress the virus before you receive chemotherapy. Without this medication, the chemotherapy can help the virus to grow and cause damage to the liver.
- Blood tumor marker tests. Serum tumor markers are tumor proteins in a person's blood. Higher levels of a serum tumor marker may be due to cancer or a noncancerous condition. Tumor marker testing is not recommended for early-stage breast cancer because the markers are not usually high, but they may be useful to monitor the growth of recurrent or metastatic disease along with symptoms and imaging tests. Tumor markers should not be used to monitor for a recurrence, as such testing does not appear to improve a patient’s chance of recovery. Learn more about tumor markers for breast cancer
- X-ray. An x-ray is a way to create a picture of the structures inside of the body, using a small amount of radiation. A chest x-ray may be used to look for cancer that has spread from the breast to the lungs.
- Bone scan. A bone scan may be used to look for spread of cancer to the bones. A radioactive dye or tracer is injected into a patient’s vein, and then the scan is performed several hours later using a special camera. The tracer collects in areas of the bone that are healing, which occurs in response to damage from the cancer cells. The areas where the tracer collects appear dark, compared to healthy bone, which appears gray. Some cancers do not cause the same healing response and will not show up on the bone scan. Areas of advanced arthritis or healing after a fracture will also appear dark.
- Computed tomography (CT or CAT) scan. A CT scan may be used to look for tumors in organs outside of the breast, such as the lung, liver, bone, and lymph nodes. A CT scan creates a three-dimensional picture of the inside of the body with a special x-ray machine. A computer combines these images into a detailed, cross-sectional view that shows abnormalities, including most tumors. A CT scan can also be used to measure the tumor’s size and if it is shrinking with treatment. A contrast dye may be injected into a patient’s vein before the scan to provide better detail.
- Positron emission tomography (PET) scan. A PET scan may also be used to find out whether the cancer has spread to organs outside of the breast. Similar to a CT scan, a PET scan is a way to create pictures of organs and tissues inside the body. A small amount of a radioactive sugar substance is injected into a patient’s vein. This sugar substance is then taken up by cells that use the most energy because they are actively dividing. Because cancer cells tend to use energy actively, they absorb more of the radioactive substance. A scanner then detects this substance to produce images of the inside of the body. Areas that are most active appear as bright spots, and the intensity of the brightness can be measured to better describe these areas. A combination PET/CT scan may also be used to measure the size of tumors and to determine the location of the bright spots more accurately. A PET/CT scan will also show any abnormalities in the bone, similar to the bone scan.
Breast cancer treatment takes different approaches depending on the conditions. The mainstay of breast cancer treatment is surgery when the tumor is localized, followed by chemotherapy (when indicated), radiotherapy, and, for ER-positive tumours, adjuvant hormonal therapy (with tamoxifen or an aromatase inhibitor). Management of breast cancer is undertaken by a multidisciplinary team based on national and international guidelines. Depending on clinical criteria (age, type of cancer, size, presence or absence of metastasis) patients are roughly divided to high risk and low risk cases, with each risk category following different rules for therapy. Treatment possibilities include radiation therapy, chemotherapy, hormone therapy, and immune therapy
PROGNOSIS
Survival rates tell you what portion of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding about the outlook. Some people will want to know the survival rates for their cancer type and stage, and some people won’t.
Survival rates are often used by doctors as a standard way of discussing a person's outlook (prognosis). Some women with breast cancer might want to know the survival statistics for people in similar situations, while others might not find the numbers helpful, or might even not want to know them.
What is a 5-year survival rate?Statistics on the outlook for a certain type and stage of cancer are often given as 5-year survival rates, but many people live longer – often much longer – than 5 years. The 5-year survival rate is the percentage of people who live at least 5 years after being diagnosed with cancer. For example, a 5-year survival rate of 90% means that an estimated 90 out of 100 people who have that cancer are still alive 5 years after being diagnosed.
Relative survival rates are a more accurate way to estimate the effect of cancer on survival. These rates compare women with breast cancer to women in the overall population. For example, if the 5-year relative survival rate for a specific type of cancer is 90%, it means that people who have that cancer are, on average, about 90% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
But remember, the 5-year relative survival rates are estimates – your outlook can vary based on a number of factors specific to you.
Survival rates don’t tell the whole storySurvival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a number of limitations to remember:
5-year relative survival rates for breast cancer, by stageThe outlook for women with breast cancer varies by the stage (extent) of the cancer. In general, the survival rates are higher for women with earlier stage cancers. But remember, the outlook for each woman is specific to her circumstances.
Survival rates are often used by doctors as a standard way of discussing a person's outlook (prognosis). Some women with breast cancer might want to know the survival statistics for people in similar situations, while others might not find the numbers helpful, or might even not want to know them.
What is a 5-year survival rate?Statistics on the outlook for a certain type and stage of cancer are often given as 5-year survival rates, but many people live longer – often much longer – than 5 years. The 5-year survival rate is the percentage of people who live at least 5 years after being diagnosed with cancer. For example, a 5-year survival rate of 90% means that an estimated 90 out of 100 people who have that cancer are still alive 5 years after being diagnosed.
Relative survival rates are a more accurate way to estimate the effect of cancer on survival. These rates compare women with breast cancer to women in the overall population. For example, if the 5-year relative survival rate for a specific type of cancer is 90%, it means that people who have that cancer are, on average, about 90% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
But remember, the 5-year relative survival rates are estimates – your outlook can vary based on a number of factors specific to you.
Survival rates don’t tell the whole storySurvival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a number of limitations to remember:
- The numbers below are among the most current available. But to get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. As treatments are improving over time, women who are now being diagnosed with breast cancer may have a better outlook than these statistics show.
- The available statistics for breast cancer do not divide survival rates by all of the sub stages, such as IA and IB. The rates for these substages are likely to be close to the rate for the overall stage. For example, the survival rate for stage IA is likely to be slightly higher than that listed for stage I, while the survival rate for stage IB would be expected to be slightly lower.
- These statistics are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that later come back or spread, for example.
- Many other factors affect a person's outlook, such as age and health, the presence of hormone receptors on the cancer cells, the treatment received, and how well the cancer responds to treatment.
5-year relative survival rates for breast cancer, by stageThe outlook for women with breast cancer varies by the stage (extent) of the cancer. In general, the survival rates are higher for women with earlier stage cancers. But remember, the outlook for each woman is specific to her circumstances.
- The 5-year relative survival rate for women with stage 0 or stage I breast cancer is close to 100%.
- For women with stage II breast cancer, the 5-year relative survival rate is about 93%.
- The 5-year relative survival rate for stage III breast cancers is about 72%. But often, women with these breast cancers can be successfully treated.
- Breast cancers that have spread to other parts of the body are more difficult to treat and tend to have a poorer outlook. Metastatic, or stage IV breast cancers, have a 5-year relative survival rate of about 22%. Still, there are often many treatment options available for women with this stage of breast cancer.
PREVENTION
Breast cancer prevention starts with healthy habits — such as limiting alcohol and staying physically active. Understand what you can do to reduce your breast cancer risk.
By Mayo Clinic StaffIf you're concerned about breast cancer, you might be wondering if there are steps you can take toward breast cancer prevention. Some risk factors, such as family history, can't be changed. However, there are lifestyle changes you can make to lower your risk.
What can I do to reduce my risk of breast cancer?Lifestyle changes have been shown in studies to decrease breast cancer risk even in high-risk women. The following are steps you can take to lower your risk:
Maintaining a healthy weight also is a key factor in breast cancer prevention.
By Mayo Clinic StaffIf you're concerned about breast cancer, you might be wondering if there are steps you can take toward breast cancer prevention. Some risk factors, such as family history, can't be changed. However, there are lifestyle changes you can make to lower your risk.
What can I do to reduce my risk of breast cancer?Lifestyle changes have been shown in studies to decrease breast cancer risk even in high-risk women. The following are steps you can take to lower your risk:
- Limit alcohol. The more alcohol you drink, the greater your risk of developing breast cancer. The general recommendation — based on research on the effect of alcohol on breast cancer risk — is to limit yourself to less than 1 drink per day as even small amounts increase risk.
- Don't smoke. Accumulating evidence suggests a link between smoking and breast cancer risk, particularly in premenopausal women. In addition, not smoking is one of the best things you can do for your overall health.
- Control your weight. Being overweight or obese increases the risk of breast cancer. This is especially true if obesity occurs later in life, particularly after menopause.
- Be physically active. Physical activity can help you maintain a healthy weight, which, in turn, helps prevent breast cancer. For most healthy adults, the Department of Health and Human Services recommends at least 150 minutes a week of moderate aerobic activity or 75 minutes of vigorous aerobic activity weekly, plus strength training at least twice a week.
- Breast-feed. Breast-feeding might play a role in breast cancer prevention. The longer you breast-feed, the greater the protective effect.
- Limit dose and duration of hormone therapy. Combination hormone therapy for more than three to five years increases the risk of breast cancer. If you're taking hormone therapy for menopausal symptoms, ask your doctor about other options. You might be able to manage your symptoms with nonhormonal therapies and medications. If you decide that the benefits of short-term hormone therapy outweigh the risks, use the lowest dose that works for you and continue to have your doctor monitor the length of time you are taking hormones.
- Avoid exposure to radiation and environmental pollution. Medical-imaging methods, such as computerized tomography, use high doses of radiation. While more studies are needed, some research suggests a link between breast cancer and radiation exposure. Reduce your exposure by having such tests only when absolutely necessary.
Maintaining a healthy weight also is a key factor in breast cancer prevention.
3 Chromosomal Abnormalities
Jacobsen Syndrome
Down Syndrome
Klinefelter
Down Syndrome
Klinefelter
Definition
Jacobsen
Jacobsen syndrome, also known as 11q deletion disorder, results from a loss of genetic material from the end of the long arm of chromosome 11. Signs and symptoms of this condition vary, but most individuals experience delayed development in motor skills and speech, cognitive impairments, learning difficulties, and some behavioral problems.
https://ghr.nlm.nih.gov/condition
https://ghr.nlm.nih.gov/condition
Down
Down syndrome is a developmental disorder caused by an extra copy of chromosome 21 (which is why the disorder is also called "trisomy 21"). Having an extra copy of this chromosome means that individuals have three copies of each of its genes instead of two, making it difficult for cells to properly control how much protein is made. Producing too much or too little protein can have serious consequences. Genes on chromosome 21 that specifically contribute to the various symptoms of Down syndrome are now being identified.
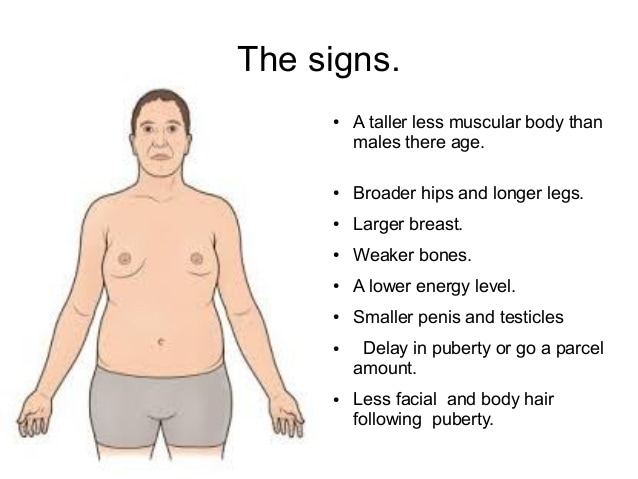
Klinefelter
47, XXY (or XXY) is a genetic condition caused when someone has two X chromosomes and one Y chromosome. Males normally have an X chromosome and a Y chromosome (46, XY), and females normally have two X chromosomes (46, XX).
Because people with an XXY chromosome arrangement have a Y chromosome, they are considered genetic males. Most XXY individuals develop as males, often not knowing they have an extra chromosome. Some will develop the varied and often subtle characteristics associated with Klinefelter syndrome. And a small proportion will develop as intersex (between male and female) or female. Physical characteristics may appear around the time of puberty, when gender identity and sexual characteristics begin to take shape.
Similar conditions are caused by additional X chromosomes (48, XXXY; 49, XXXXY), but they are much more rare. The more X chromosomes a person has, the stronger the physical characteristics and health problems tend to be, including intellectual disability.
https://learn.genetics.utah.edu/content/disorders/chromosomal/
Because people with an XXY chromosome arrangement have a Y chromosome, they are considered genetic males. Most XXY individuals develop as males, often not knowing they have an extra chromosome. Some will develop the varied and often subtle characteristics associated with Klinefelter syndrome. And a small proportion will develop as intersex (between male and female) or female. Physical characteristics may appear around the time of puberty, when gender identity and sexual characteristics begin to take shape.
Similar conditions are caused by additional X chromosomes (48, XXXY; 49, XXXXY), but they are much more rare. The more X chromosomes a person has, the stronger the physical characteristics and health problems tend to be, including intellectual disability.
https://learn.genetics.utah.edu/content/disorders/chromosomal/
Illustration

Jacobsen |

Down |
Klinefelter |
Frequency
Jacobsen
Jacobsen syndrome is a rare congenital condition that’s caused by the deletion of several genes in chromosome 11. It’s sometimes called partial monosomy 11q. It occurs in about 1 in 100,000 newborns.
http://www.healthline.com/health/jacobsen-syndrome
http://www.healthline.com/health/jacobsen-syndrome
Down
Down syndrome occurs in about 1 in 800 newborns. About 5,300 babies with Down syndrome are born in the United States each year, and approximately 200,000 people in this country have the condition. Although women of any age can have a child with Down syndrome, the chance of having a child with this condition increases as a woman gets older.
Klinefelter
Klinefelter syndrome affects 1 in 500 to 1,000 newborn males. Most variants of Klinefelter syndrome are much rarer, occurring in 1 in 50,000 or fewer newborns.
Researchers suspect that Klinefelter syndrome is underdiagnosed because the condition may not be identified in people with mild signs and symptoms. Additionally, the features of the condition vary and overlap significantly with those of other conditions.
Researchers suspect that Klinefelter syndrome is underdiagnosed because the condition may not be identified in people with mild signs and symptoms. Additionally, the features of the condition vary and overlap significantly with those of other conditions.
Inheritance Pattern
Jacobsen
Most cases of Jacobsen syndrome are not inherited. They result from a chromosomal deletion that occurs as a random event during the formation of reproductive cells (eggs or sperm) or in early fetal development. Affected people typically have no history of the disorder in their family, although they can pass the chromosome deletion to their children.
Between 5 and 10 percent of people with Jacobsen syndrome inherit the chromosome abnormality from an unaffected parent. In these cases, the parent carries a chromosomal rearrangement called a balanced translocation, in which a segment from chromosome 11 has traded places with a segment from another chromosome. In a balanced translocation, no genetic material is gained or lost. Balanced translocations usually do not cause any health problems; however, they can become unbalanced as they are passed to the next generation.
Children who inherit an unbalanced translocation can have a chromosomal rearrangement with some missing genetic material and some extra genetic material. Individuals with Jacobsen syndrome who inherit an unbalanced translocation are missing genetic material from the end of the long arm of chromosome 11 and have extra genetic material from another chromosome. These chromosomal changes result in the health problems characteristic of this disorder.
https://ghr.nlm.nih.gov/condition
Between 5 and 10 percent of people with Jacobsen syndrome inherit the chromosome abnormality from an unaffected parent. In these cases, the parent carries a chromosomal rearrangement called a balanced translocation, in which a segment from chromosome 11 has traded places with a segment from another chromosome. In a balanced translocation, no genetic material is gained or lost. Balanced translocations usually do not cause any health problems; however, they can become unbalanced as they are passed to the next generation.
Children who inherit an unbalanced translocation can have a chromosomal rearrangement with some missing genetic material and some extra genetic material. Individuals with Jacobsen syndrome who inherit an unbalanced translocation are missing genetic material from the end of the long arm of chromosome 11 and have extra genetic material from another chromosome. These chromosomal changes result in the health problems characteristic of this disorder.
https://ghr.nlm.nih.gov/condition
Down
Most cases of Down syndrome are not inherited. When the condition is caused by trisomy 21, the chromosomal abnormality occurs as a random event during the formation of reproductive cells in a parent. The abnormality usually occurs in egg cells, but it occasionally occurs in sperm cells. An error in cell division called nondisjunction results in a reproductive cell with an abnormal number of chromosomes. For example, an egg or sperm cell may gain an extra copy of chromosome 21. If one of these atypical reproductive cells contributes to the genetic makeup of a child, the child will have an extra chromosome 21 in each of the body's cells.
People with translocation Down syndrome can inherit the condition from an unaffected parent. The parent carries a rearrangement of genetic material between chromosome 21 and another chromosome. This rearrangement is called a balanced translocation. No genetic material is gained or lost in a balanced translocation, so these chromosomal changes usually do not cause any health problems. However, as this translocation is passed to the next generation, it can become unbalanced. People who inherit an unbalanced translocation involving chromosome 21 may have extra genetic material from chromosome 21, which causes Down syndrome.
Like trisomy 21, mosaic Down syndrome is not inherited. It occurs as a random event during cell division early in fetal development. As a result, some of the body's cells have the usual two copies of chromosome 21, and other cells have three copies of this chromosome.
People with translocation Down syndrome can inherit the condition from an unaffected parent. The parent carries a rearrangement of genetic material between chromosome 21 and another chromosome. This rearrangement is called a balanced translocation. No genetic material is gained or lost in a balanced translocation, so these chromosomal changes usually do not cause any health problems. However, as this translocation is passed to the next generation, it can become unbalanced. People who inherit an unbalanced translocation involving chromosome 21 may have extra genetic material from chromosome 21, which causes Down syndrome.
Like trisomy 21, mosaic Down syndrome is not inherited. It occurs as a random event during cell division early in fetal development. As a result, some of the body's cells have the usual two copies of chromosome 21, and other cells have three copies of this chromosome.
Klinefelter
Klinefelter syndrome and its variants are not inherited; these chromosomal changes usually occur as random events during the formation of reproductive cells (eggs and sperm) in a parent. An error in cell division called nondisjunction results in a reproductive cell with an abnormal number of chromosomes. For example, an egg or sperm cell may gain one or more extra copies of the X chromosome as a result of nondisjunction. If one of these atypical reproductive cells contributes to the genetic makeup of a child, the child will have one or more extra X chromosomes in each of the body's cells.
Mosaic 46,XY/47,XXY is also not inherited. It occurs as a random event during cell division early in fetal development. As a result, some of the body's cells have one X chromosome and one Y chromosome (46,XY), and other cells have an extra copy of the X chromosome (47,XXY).
https://ghr.nlm.nih.gov/condition
Diagnosis and Management
Jacobsen
JACOBSENThese resources address the diagnosis or management of Jacobsen syndrome:
- 11q Research & Resource Group: Concerns and Recommendations
- Genetic Testing Registry: 11q partial monosomy syndrome
- Unique: Chromosome 11q Deletion Disorder: Jacobsen Syndrome (PDF)
Down
These resources address the diagnosis or management of Down syndrome:
- Genetic Testing Registry: Complete trisomy 21 syndrome
- National Down Syndrome Congress: Health Care
- National Down Syndrome Congress: Speech and Language
- National Down Syndrome Society: Health Care
- National Down Syndrome Society: Therapies and Development
Klinefelter
These resources address the diagnosis or management of Klinefelter syndrome:
https://ghr.nlm.nih.gov/condition
- Genetic Testing Registry: Klinefelter's syndrome, XXY
- MedlinePlus Encyclopedia: Klinefelter Syndrome
- MedlinePlus Encyclopedia: Testicular Failure
https://ghr.nlm.nih.gov/condition
Prognosis
Jacobsen
Jacobsen syndrome can result in a large number of serious complications.
Learning disabilities affect about 97 percent of individuals with Jacobsen syndrome. These learning difficulties are typically mild to moderate. They can be severe.
Bleeding disorders are a serious but common complication of Jacobsen syndrome. About 88 percent of children with Jacobsen syndrome are born with Paris-Trousseau syndrome. This is a bleeding disorder that makes you bruise easily or bleed a lot. This can put you at a risk for internal bleeding. Even nosebleeds or blood work can result in heavy blood loss.
Heart conditions are also a common complication. About 56 percent of children with Jacobsen syndrome are born with heart conditions. Some of these will need surgery to be treated. About 20 percent of children with Jacobsen will die of heart complications before they’re 2 years old. Common heart defects include:
Because some children with Jacobsen syndrome are immunodeficient, they may be much more susceptible to infections. Ear and sinus infections are especially common. Some children will have such severe ear infections they may get hearing loss.
http://www.healthline.com/health/jacobsen-syndrome#Complications5
Learning disabilities affect about 97 percent of individuals with Jacobsen syndrome. These learning difficulties are typically mild to moderate. They can be severe.
Bleeding disorders are a serious but common complication of Jacobsen syndrome. About 88 percent of children with Jacobsen syndrome are born with Paris-Trousseau syndrome. This is a bleeding disorder that makes you bruise easily or bleed a lot. This can put you at a risk for internal bleeding. Even nosebleeds or blood work can result in heavy blood loss.
Heart conditions are also a common complication. About 56 percent of children with Jacobsen syndrome are born with heart conditions. Some of these will need surgery to be treated. About 20 percent of children with Jacobsen will die of heart complications before they’re 2 years old. Common heart defects include:
- holes between the left and right lower chambers
- abnormalities on the left side of the heart
- hypoplastic left heart syndrome, a defect that affects blood flow through the heart
- having a single kidney
- double ureters (the tubes leading from the kidneys to the bladder)
- hydroneprosis, or swelling
- cysts
- blocked or narrow anus
- constipation
- intestinal obstruction
- missing parts of the GI tract
- abnormal positioning of the gut
Because some children with Jacobsen syndrome are immunodeficient, they may be much more susceptible to infections. Ear and sinus infections are especially common. Some children will have such severe ear infections they may get hearing loss.
http://www.healthline.com/health/jacobsen-syndrome#Complications5
Down
The life expectancy for people with Down Syndrome has increased substantially. In 1929, the average life span of a person with Down Syndrome was nine years. Today, it is common for a person with Down Syndrome to live to age 50 and beyond.
In addition to living longer, people with Down Syndrome are now living fuller, richer lives than ever before as family members and contributors to their community. Many people with Down Syndrome form meaningful relationships and eventually marry.
Now that people with Down Syndrome are living longer, the needs of adults with Down syndrome are receiving greater attention. With assistance from family and caretakers, many adults with Down Syndrome have developed the skills required to hold jobs and to live semi-independently.’
http://www.mychildwithoutlimits.org/understand/down-syndrome/down-syndrome-prognosis/
In addition to living longer, people with Down Syndrome are now living fuller, richer lives than ever before as family members and contributors to their community. Many people with Down Syndrome form meaningful relationships and eventually marry.
Now that people with Down Syndrome are living longer, the needs of adults with Down syndrome are receiving greater attention. With assistance from family and caretakers, many adults with Down Syndrome have developed the skills required to hold jobs and to live semi-independently.’
http://www.mychildwithoutlimits.org/understand/down-syndrome/down-syndrome-prognosis/
Klinefelter
Men with Klinefelter syndrome are at increased risk for certain medical problems. These medical problems include:
http://genetics.emedtv.com/klinefelter-syndrome/prognosis-of-klinefelter-syndrome.html
- Autoimmune diseases, including type 1 diabetes, lupus, and hypothyroidism
- Male breast cancer
- Non-Hodgkin's lymphoma
- Obesity
- Osteoporosis.
http://genetics.emedtv.com/klinefelter-syndrome/prognosis-of-klinefelter-syndrome.html

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}